Emergency card
Care and emergency card established for doctors and emergency physicians and Crigler-Najjar patients.
All the recommendations and precautions to be taken in an emergency.
(click on the image to download the card)

Bilirubin / albumin molar ratio
WHAT IS THE BILIRUBUN TO ALBUMIN MOLAR RATIO?
The bilirubin to albumin molar ratio is the number of bilirubin molecules present divided by the number of albumin molecules present. When the number of molecules is equal this is referred to as a molar ratio of one. When the molar ratio is close to or greater than one, there will be dangerous “free” bilirubin molecules.
For people with fully functioning livers, the molar ratio is only about 0.01. This is only about one hundredth of the very dangerous level. For people with Gilberts Syndrome the ratio is about 0.1 or about one tenth of the very dangerous level.
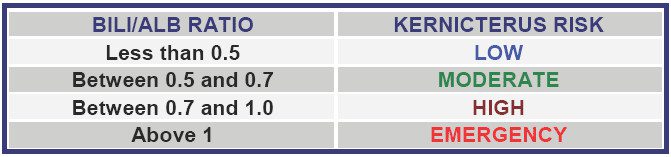
For people with Crigler-Najjar Syndrome, the molar ratio of bilirubin to albumin is higher, but should be kept as low as possible. A molar ratio of 0.5 (half as many bilirubin molecules as albumin molecules) is considered relatively safe. Molar ratios above 0.7 require medical supervision and perhaps medical intervention. Molar ratios approaching 1 are dangerous and require emergency treatment to increase albumin concentration and decrease bilirubin concentration.
Because the albumin level for people obtaining good nutrition is normally within the range 35-55 grams per litre (3.5-5.5 g/dl), the molecular ratio depends mainly on the serum bilirubin concentration.
In emergency situations due to illness or accident or situations where the bilirubin concentration becomes high, the molar ratio is of critical importance. Frequent measurement of bilirubin and albumin concentrations, correct calculation of the molar ratios, and providing appropriate medical responses is essential.
HOW DOES ALBUMIN PROVIDE PROTECTION?
In well-nourished individuals the blood normally has an albumin concentration in the range 35 to 55 grams/litre. Albumin is a molecule with a molecular weight more than one hundred times that of bilirubin. It has binding sites where bilirubin molecules can and do attach themselves. Combined bilirubin/albumin molecules are too large to pass through the blood-brain barrier and thus the brain can be protected.
To visualise this it is possible to think of bilirubin having the volume of a golf ball and albumin the volume of a soccer ball. If the blood brain barrier membrane is thought of as the equivalent of the net of a soccer goal, it will be realised that the golf ball by itself could pass through the net, but it could not do so if it were firmly attached to a soccer ball.
In people with normal glucuronyl transferase production, the numbers of albumin molecules present in the blood provide many more binding sites than the number of bilirubin molecules present. As a result, virtually all of the bilirubin is attached to albumin and there is little, if any, of the dangerous so called “free” (not bound to albumin) bilirubin.
If bilirubin is not removed from the body, it builds up, and starts occupying more and more of the available albumin binding sites. Eventually it uses up virtually all the albumin sites and dangerous “free” bilirubin accumulates to do its damage.
It will be appreciated that the ratio of bilirubin molecules to albumin molecules (the molar ratio) in the blood is an important factor in the management of Crigler-Najjar Syndrome, particularly in emergency situations.
Orphanet Emergency
Orphanet Urgences, portal for rare diseases and orphan drugs, is a collection of practical recommendations for the management of patients suffering from a rare disease and requiring urgent medical care.
It is intended for emergency physicians, whether they intervene at the scene of the emergency or within hospital emergencies.
Orphanet web portal : https://www.orpha.net/consor/cgi-bin/Disease_Emergency.php?lng=EN