An ultra orphan disease
Crigler-Najjar syndrome (CNS), named after Dr John Fielding Crigler and Dr Victor Assad Najjar who discovered this disease in the 50s is an extremely rare genetic disease, less than 1 in 1 000 000 births.
Less than 20 cases in France and only a few hundred worldwide. It is an autosomique récessif disorder and it appears in the first days of life and persists thereafter.
It occurs when the enzyme that normally converts bilirubin into a form that can easily be removed from the body does not work correctly When this enzyme does not work, bilirubin can build up in the body causing an intense and chronic jaundice (yellow discoloration of skin and the sclera of the eyes).
At a high level, the bilirubine becomes toxic and can reach the brains provoking Kernicterius with severe neurological troubles rapidly leading to death. When the enzymatic activity is absent, it is called Crigler-Najjar type1 (CN1). If there is a very low activity, it is the type2 of the disease (CN2). Crigler-Najjar type 1 patients can survive thanks to a daily treatment by phototherapy .
Clinical data of CNS are described by Pr Labrune : http://www.orpha.net/consor/www/cgi-bin/OC_Exp.php?lng=EN&Expert=205
Treatment:
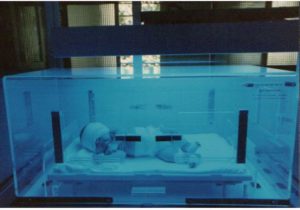
Previously, CN patients died very quickly after birth. But, in the 70s, it was found that a special bleu light with a wavelenth around 460nm was able to degrade bilirubine.
Phototherapy (PT) was born and is now commonly used to treate newborn jaundice and also to keep CN children in life . It’s the only way to try to maintain their bilirubin concentration in blood under 350µmol (reference range for total bilirubin <10µmol/L), and the bilirubine/albumine ratio under 0,6 for a a child under 1year old and 0,7 later.
Calculation of bilirubin / albumin molar ratio
Bilirubine being produced uncesselessly, CN1 patients need to be exposed daily to hudge photherapy devices at least 10-12 hours, every day of their life.
The slightest infection, cold, wounding, bruise, fracture, burning, constipation, dehydration, surgery, stress, fasting, fatigue, use of certain medicine…. can induce a sudden increase of the bilirubin, which then implies a more important exposition to PT: 13, 15 hours, even more according to the importance of the infection. A low calorie diet (400 calories per 24hr) can increase the bilirubin of about 33% (see canadian study).
See the care and emergency card.
Despite this very constraining treatment, patients have a permanent risk of developping kernicterius at any age of life. Unfortunately accidents occur, and some of them have developped severe neurological disorders or are highly handicaped or regrettably are no longer alive.
Phototherapy is now used very frequently to treat the newborn jaundice.
It has become a quite common practice. But which mom, to whom the baby was taken right after the delivery, to be put under such a device, naked and wrapped up eyes during 24 or 48 hours, could not cry seen her baby so.
Then imagine when your child has to live all his (her) life so!!!
The CN children risk their life every day. They are physically marked, they are very yellow, even orange, and the white of the eyes is yellow. They are permanently stared at. They are daily confronted to people looking at them, they are questionned, sometimes mocked. Some persons say to them that they are not beautiful, that yellow eyes does not exist, that they are extraterrestrials…
They sleep naked, feel cold in winter or too hot in summer because the devices heat, they don’t sleep well because of the presence of the intense light or because of the flies attracted by the light. They can also have a felling of insecurity from sleeping naked. These children have never lept in the dark, never worn pyjamas …

The consequences on the whole familly are important:
These children’s life is highly dependent of the extreme vigilence of their parents who are alone to administrate the treatment every day. They are always anxious for the life of their children and are permanently looking for the slightest increase in the coloration of their skin and eyes , in order to adapt the exposition to phototherapy and give the right dose to keep them in life.
They have to wake up many times at nights to control their child is not too cold or too hot, to verify he is well positionned under the light, or has not escaped, to control that the bandage is still on the eyes, to give him something to drink in order to avoid deshydratation etc…
CN1 patients are dependent on electricity, dependent on huge and practically un transportable devices and of the important lenghth of the exposition needed. PT is generaly delivered at night, put sometimes , especially when the child grows up and in case of un intercurrent disease, it’s not sufficient and more time must be found during the day.
Sharing evening with family, friends, go overnight, go on holidays, everything is difficult and nearly impossible.
It’s not easy for the parents to explain and make their children accept all these restrictions, especially when they become older and don’t understand why they cannot do the same thing as the others!!!
Despite the extreme rareness of this disease, research is very active and clinical trials on patients, financed by the french Telethon should start soon.
(voir les vidéos en page actualités et recherche)